My first patient of the day today chipped his front tooth biting his finger nail.


My first patient of the day today chipped his front tooth biting his finger nail.
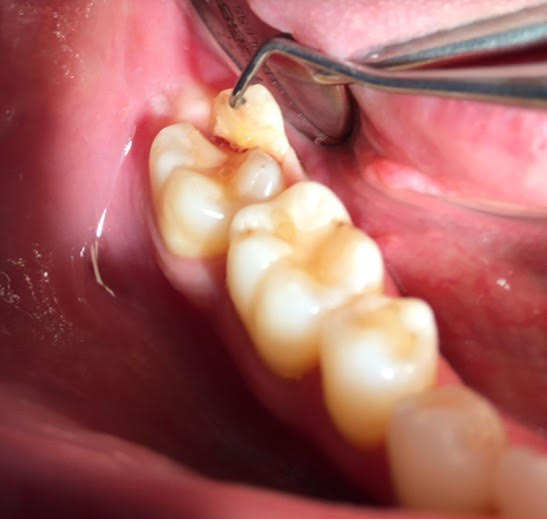
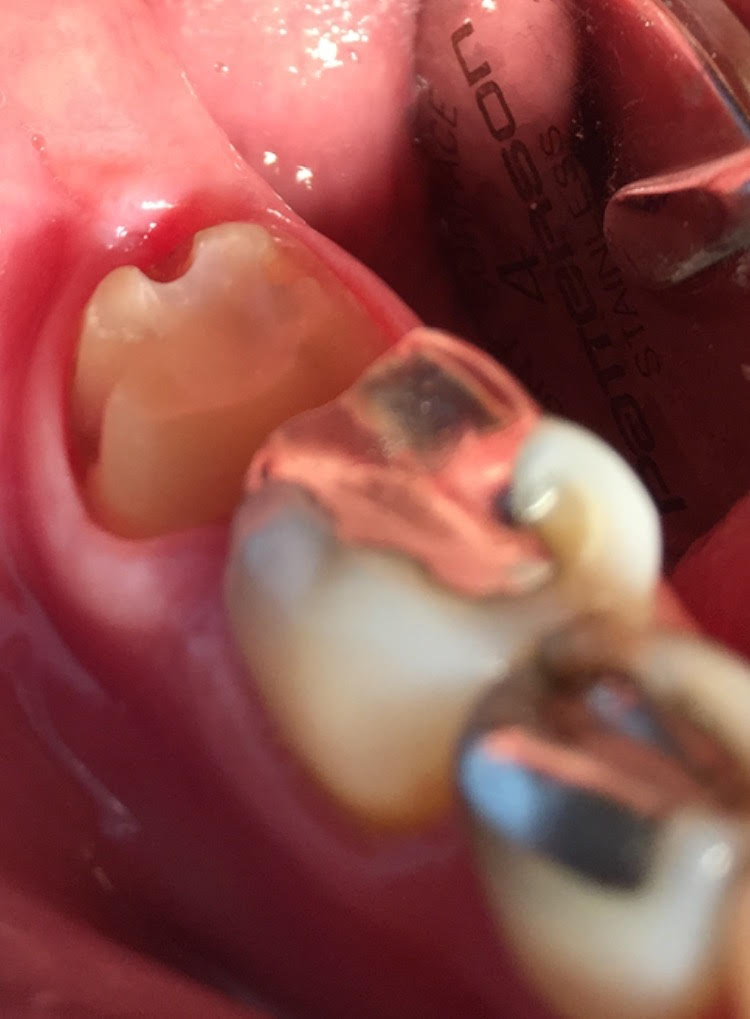
This patient cracked his molar biting a chicken bone. I was able to save the tooth, and without a root canal, but it did require a crown lengthening periodontal surgery and a crown.
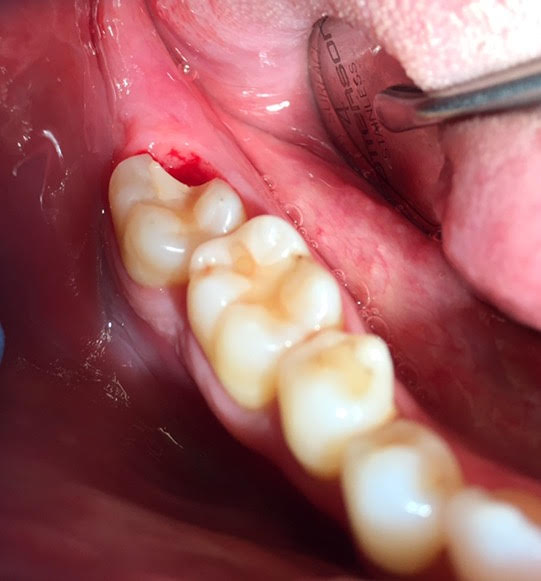
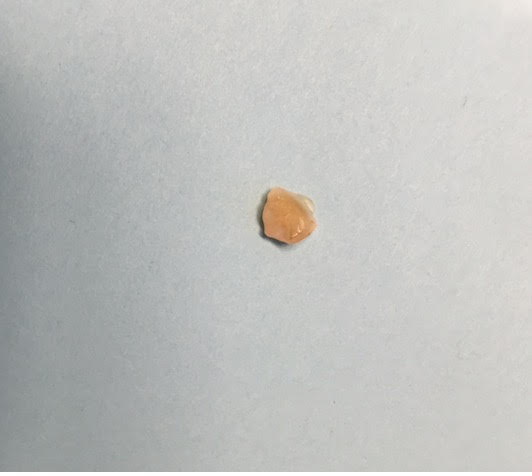

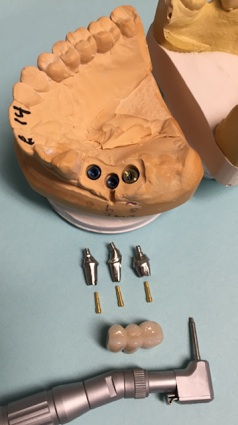
This next patient bit down on a mint candy and fractured her molar down the root. The tooth could not be restored and was extracted and we will place a dental implant.


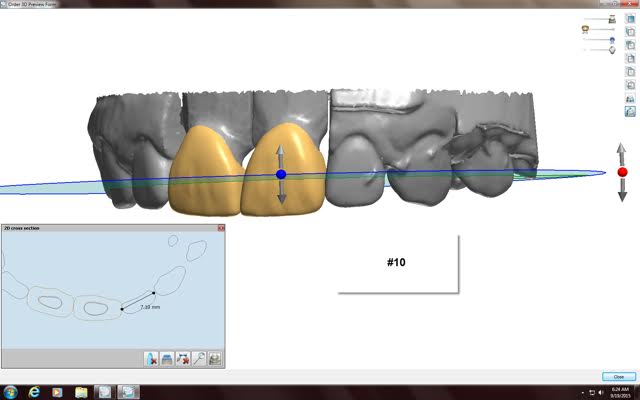
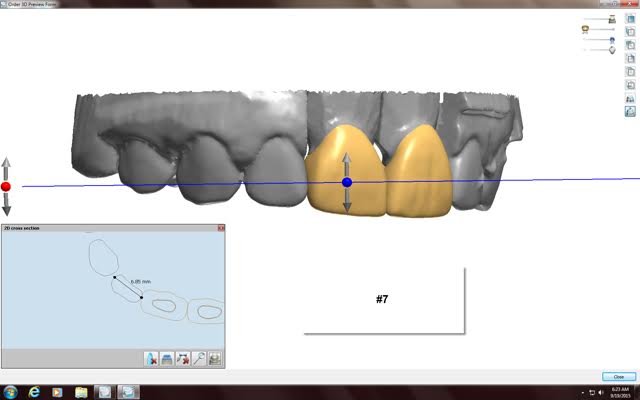
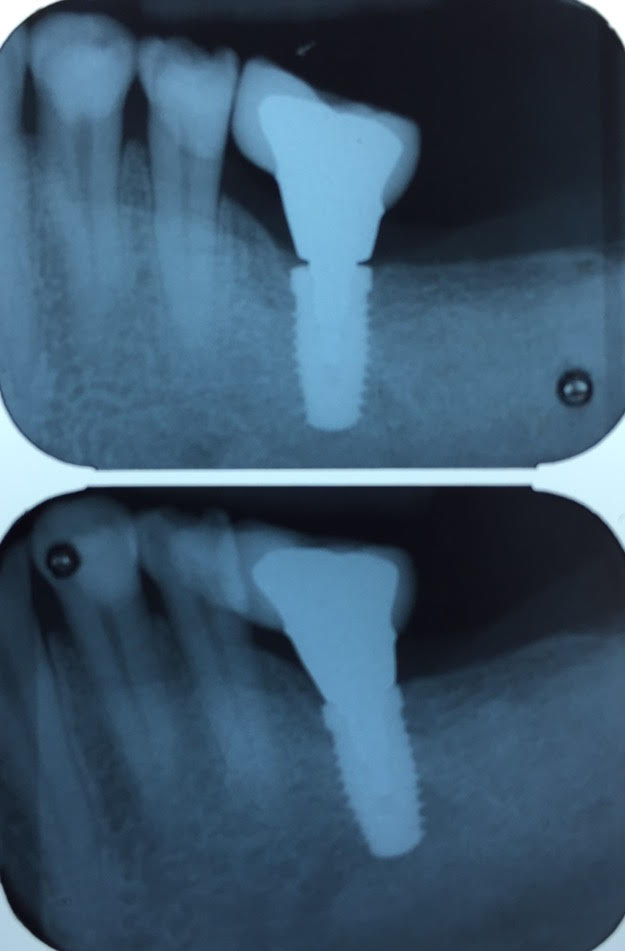
This was a challenging implant restoration case due to the alignment of implants. In order for the implant to osseointegrate firmly into the jaw bone we like to place the implants where the jaw bone is the thickest and strongest. In this case the best bone was not lined up nicely so we had to stagger the implants. I was still able to make the final implant crowns line up perfectly in the mouth.




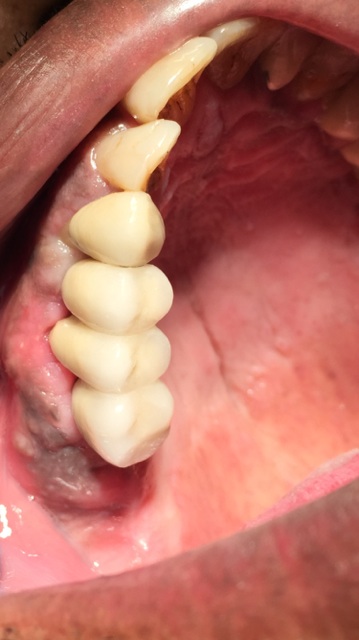
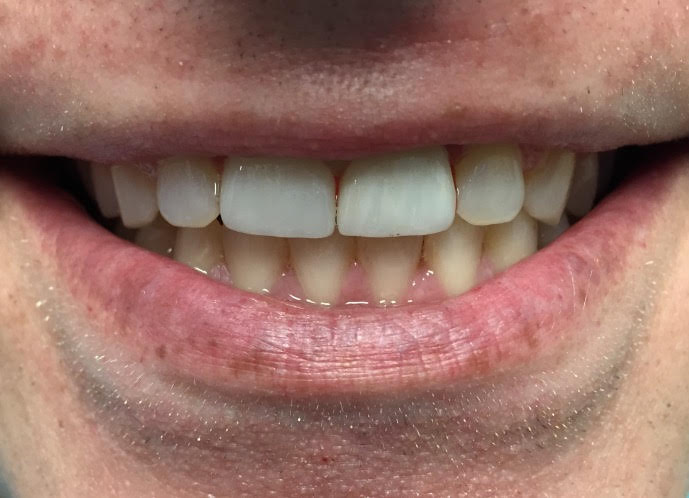
Before and After
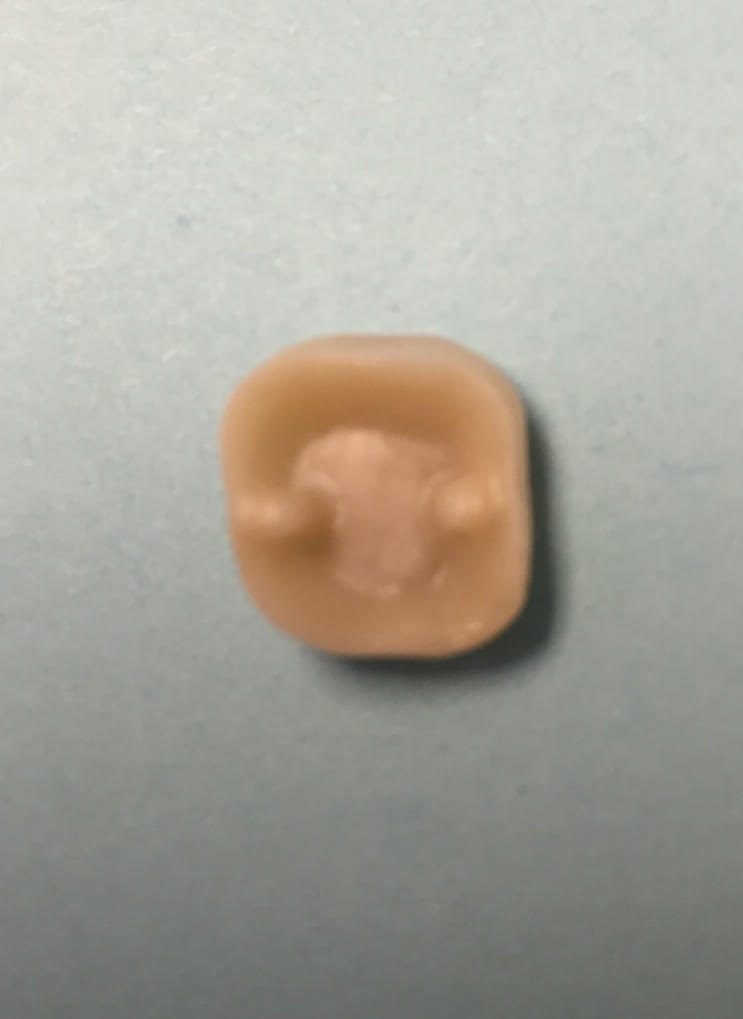
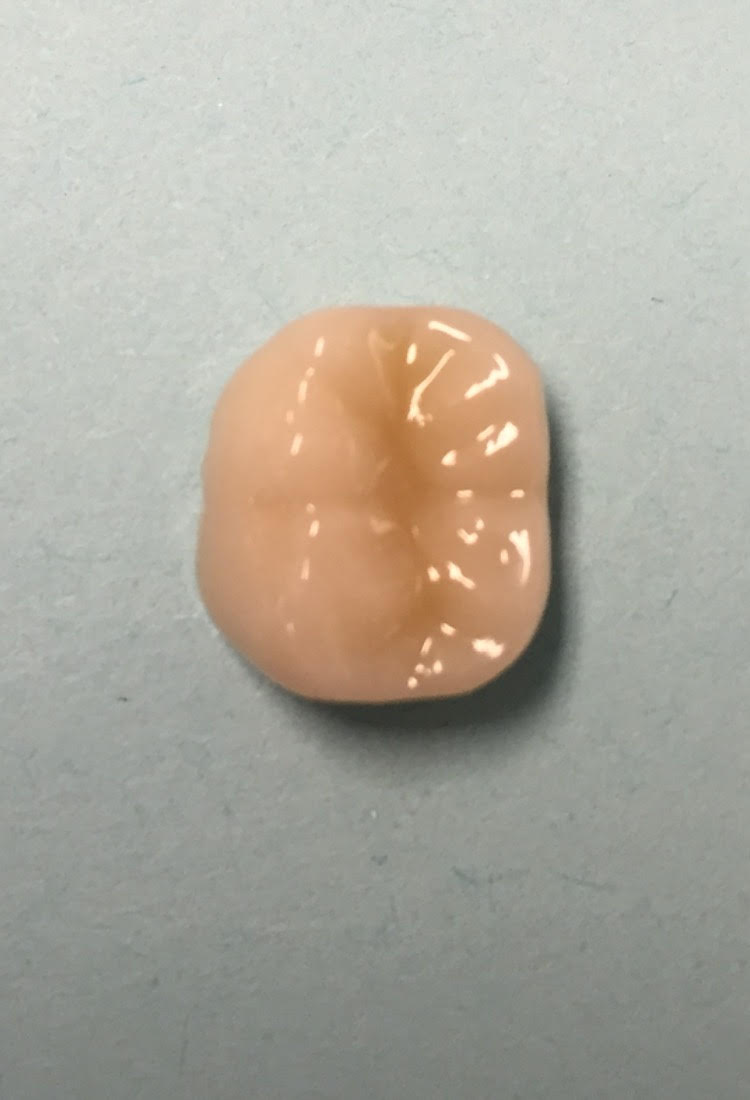
On these 2 crowns, the first porcelain and second gold, that I did last week in my office I show how I place retention grooves in my crown preparations to help lock my crowns in. These grooves prevent rotation and help secure the crowns in place. These slots allows for more surface area for the cement and results in a longer lasting restoration that holds firmly in place. This is especially important in short weak teeth. With this technique I am able to save teeth that otherwise would need to be extracted or require periodontal crown lengthening surgery.







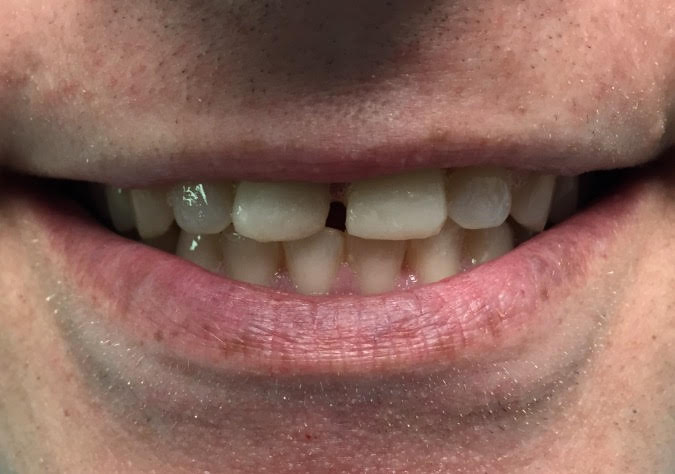
The first patient was concerned about his broken down front upper teeth and the gap between the teeth.
The next patient broke her lateral incisor tooth. It is very dark since it was traumatized and had a root canal many years ago.


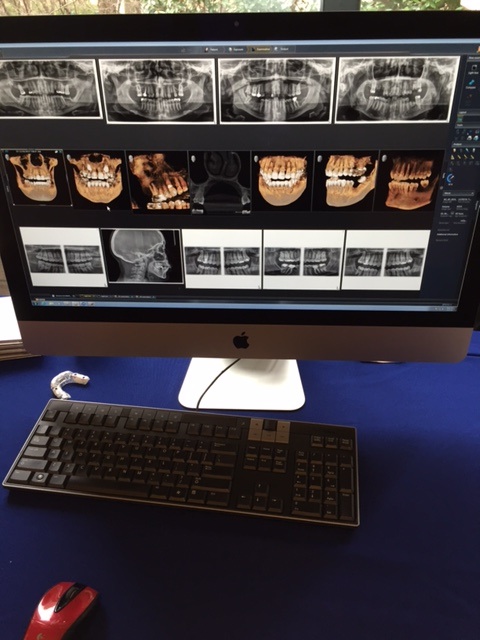
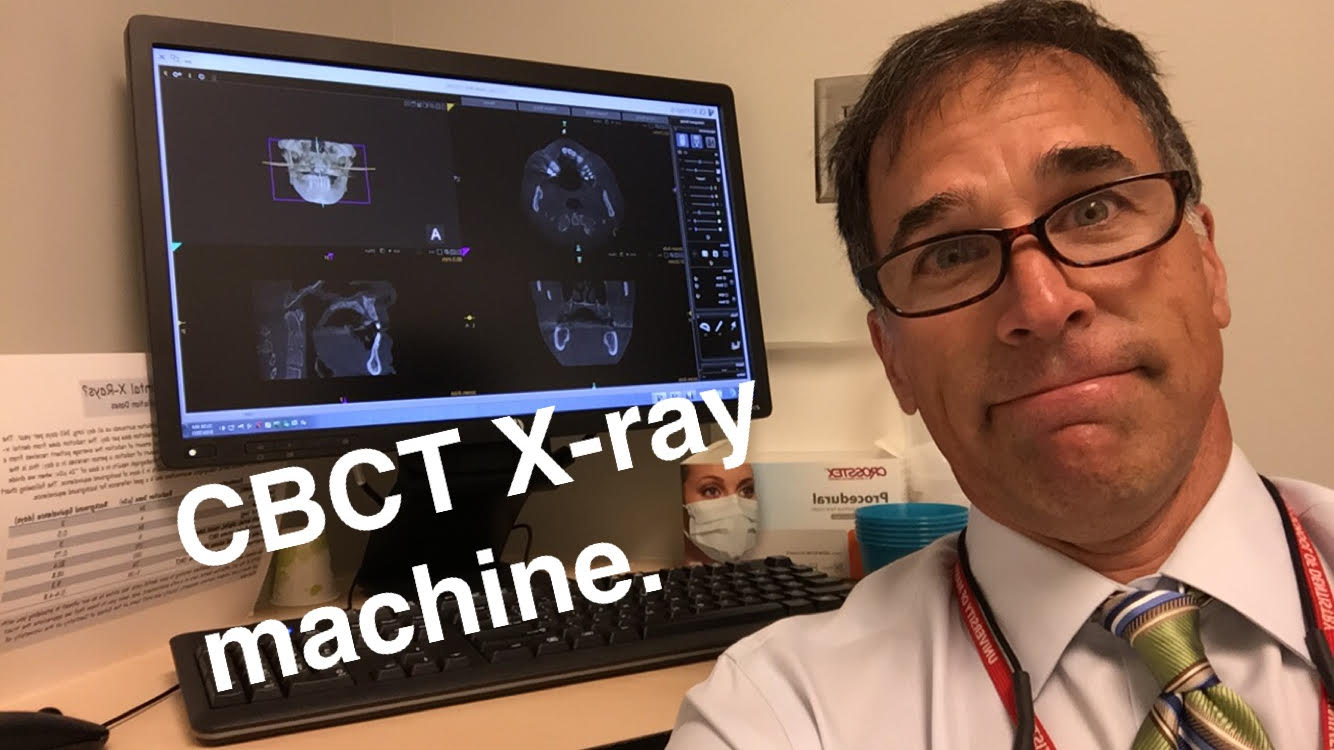
CBCT systems used by dental professionals rotate around the patient, capturing data using a cone-shaped X-ray beam. This data is used to reconstruct a three-dimensional (3D) image of the of the patient’s head and neck. CBCT uses more radiation than regular dental teeth x-rays, but still less than 10% of the radiation used in conventional medical CT scan of the same area.
This is the Carestream 9300 Imaging machine we have at the University of Maryland Dental School. I mostly use this to plan dental implant placement.
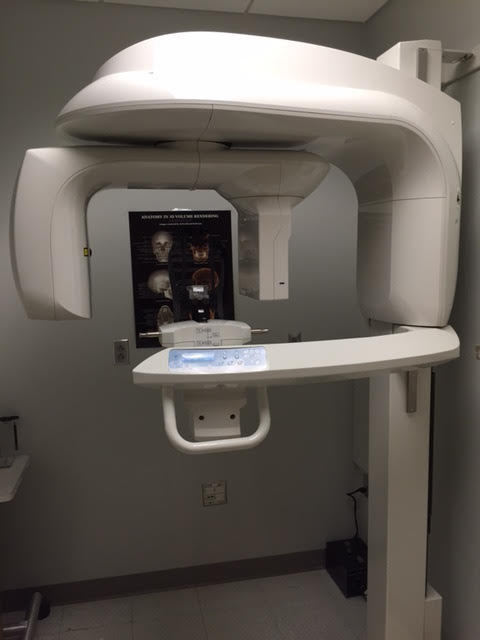
Dentists use Cone Beam CT imaging for the following:• 3-D observation of overall oral/facial bony characteristics, allowing easier diagnosis and placement of dental implants • Surgical guide fabrication for implant placement • 3-D observation of teeth for endodontic diagnosis and treatment • Diagnosis and treatment of tooth impactions • Identification of inferior alveolar nerve and mental foramen location • Identification of the location of the maxillary sinus • Identification of the presence of odontogenic lesions • Trauma evaluation and treatment • Analysis of temporomandibular joint characteristics leading to diagnosis and treatment • Integration with CAD/CAM devices for fabrication of prosthodontics or orthodontic appliances • Identification for referral of numerous conditions or diseases not normally within the realm of dentistry, but that can be shown on typical cone beam images.
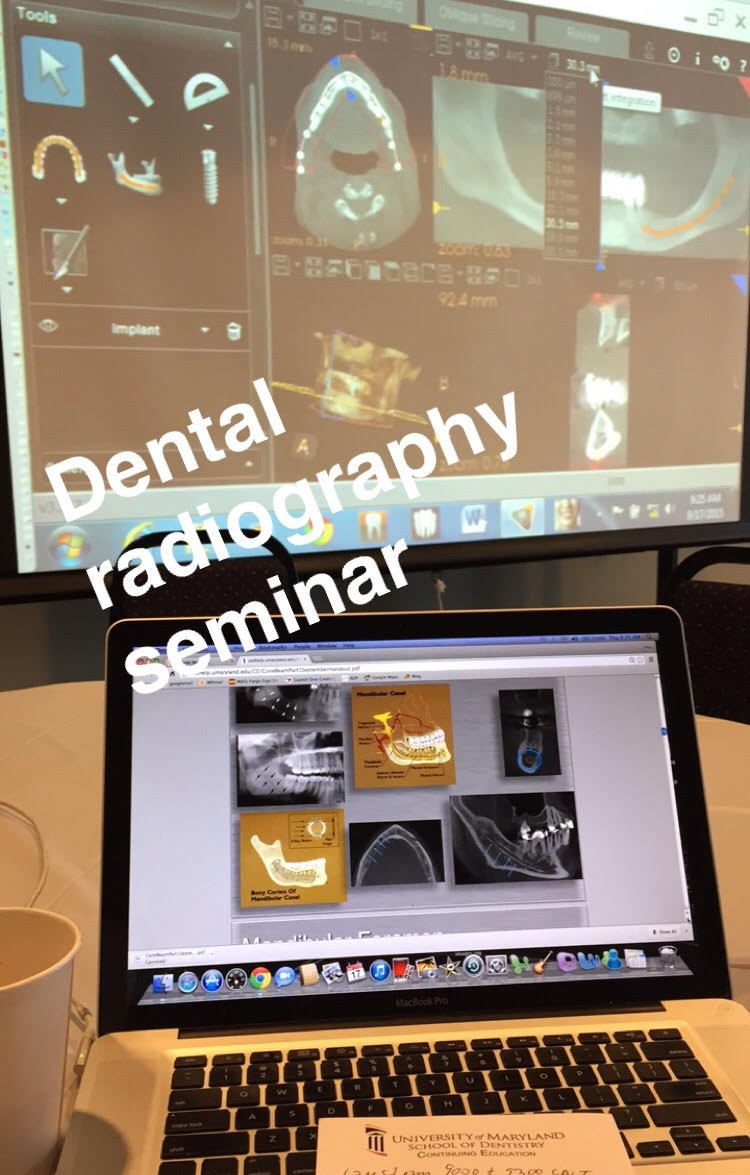

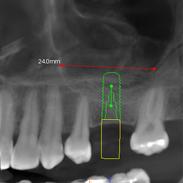
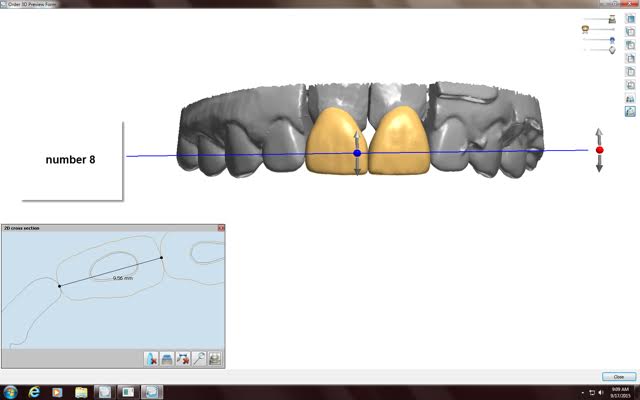
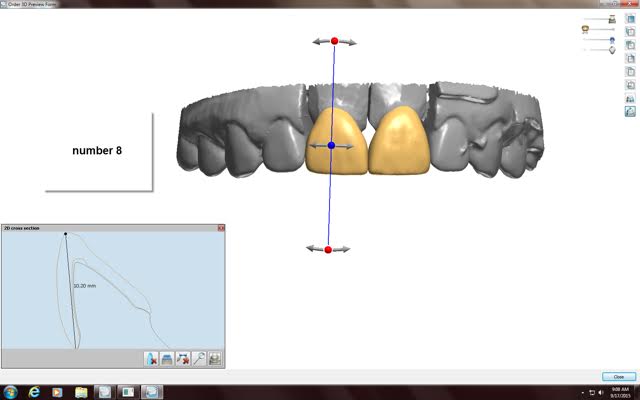
These last 2 pictures show how we use information obtained from the Cone Beam CT to plan placement of dental implants.

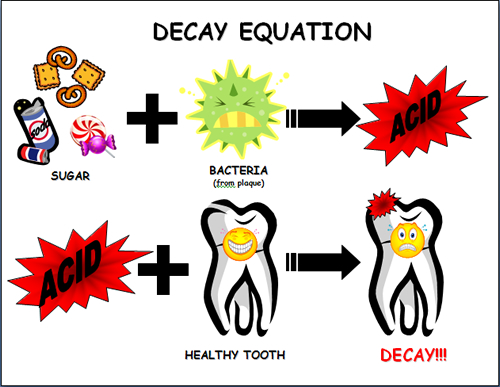
It is true that sugar does cause cavities, but it’s not the sugar directly. The naturally occurring streptococcus bacteria that live in our mouths consume the sugar, ferment it, and produce acid such as lactic acid. It is these acids that cause teeth demineralization and the formation of cavities. So it is actually the acid from the bacteria in plaque in our mouth that eats the holes in our teeth causing cavities.
Here’s the interesting part, it’s not the total amount of sugar we eat, but the total amount of time the sugar is in contact with our teeth. It is preferable to have a piece of pumpkin pie with a scoop of ice cream for Thanksgiving dessert, than sip on a soda all afternoon. It is better to have a few sugar cookies, or slice of Christmas apple pie, than to repeatedly sip coffee with sugar all morning long. One Altoids mint or cough drop per hour throughout the day is ten times more cavity producing than 1 big piece of cake for dessert, even though the cake has much more sugar and calories.
The repeated cycles of eating sugar and acid formation is what is the key. It is the frequency, or the amount of time the sugar is in the mouth, not the total amount of sugar. So do enjoy a few scrumptious (and quick) holiday desserts, just please make sure to brush and floss after every meal and visit your dentist regularly. Happy Holidays!!!
Philip A. Gentry, DDS, FAGD
Sincerely,




This patient fractured the lingual side of his first molar tooth biting down on a Skittle candy. Dr. Gentry was able to restore the tooth with a porcelain crown and was able to avoid a root canal and crown lengthening periodontal surgery.


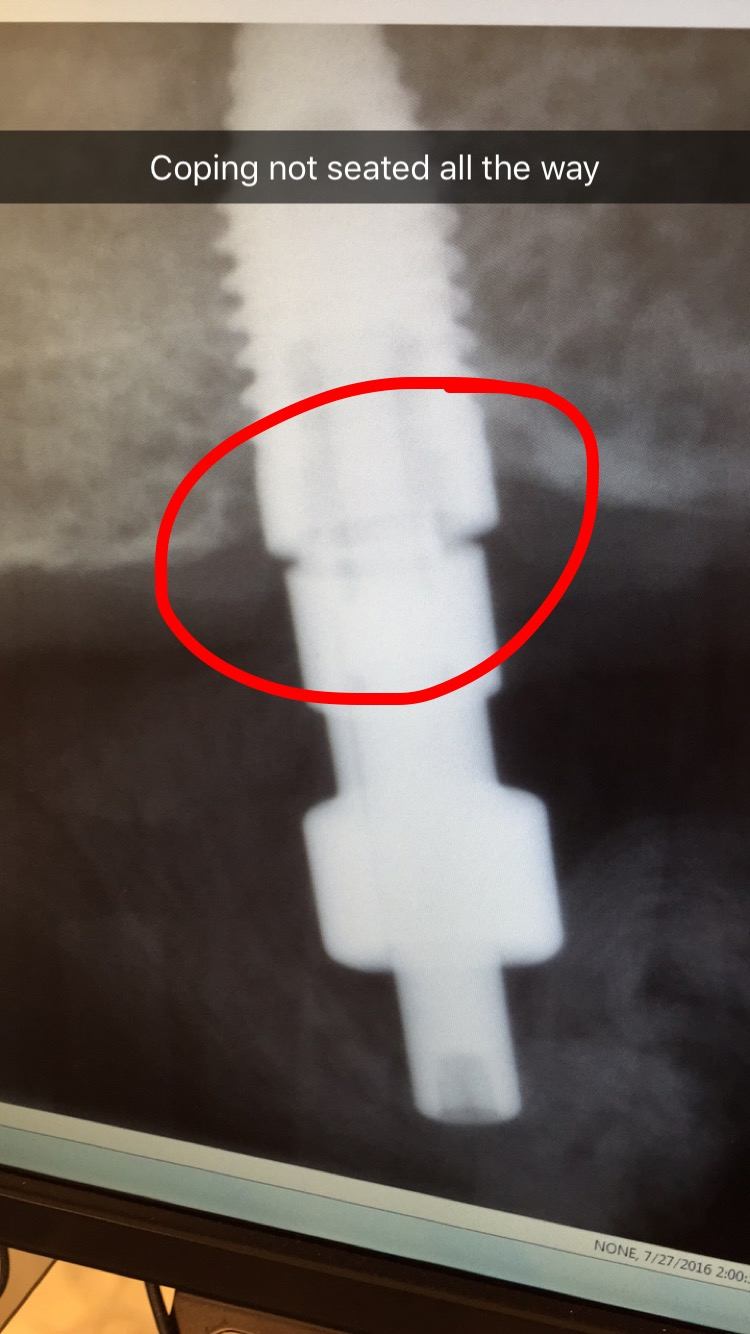
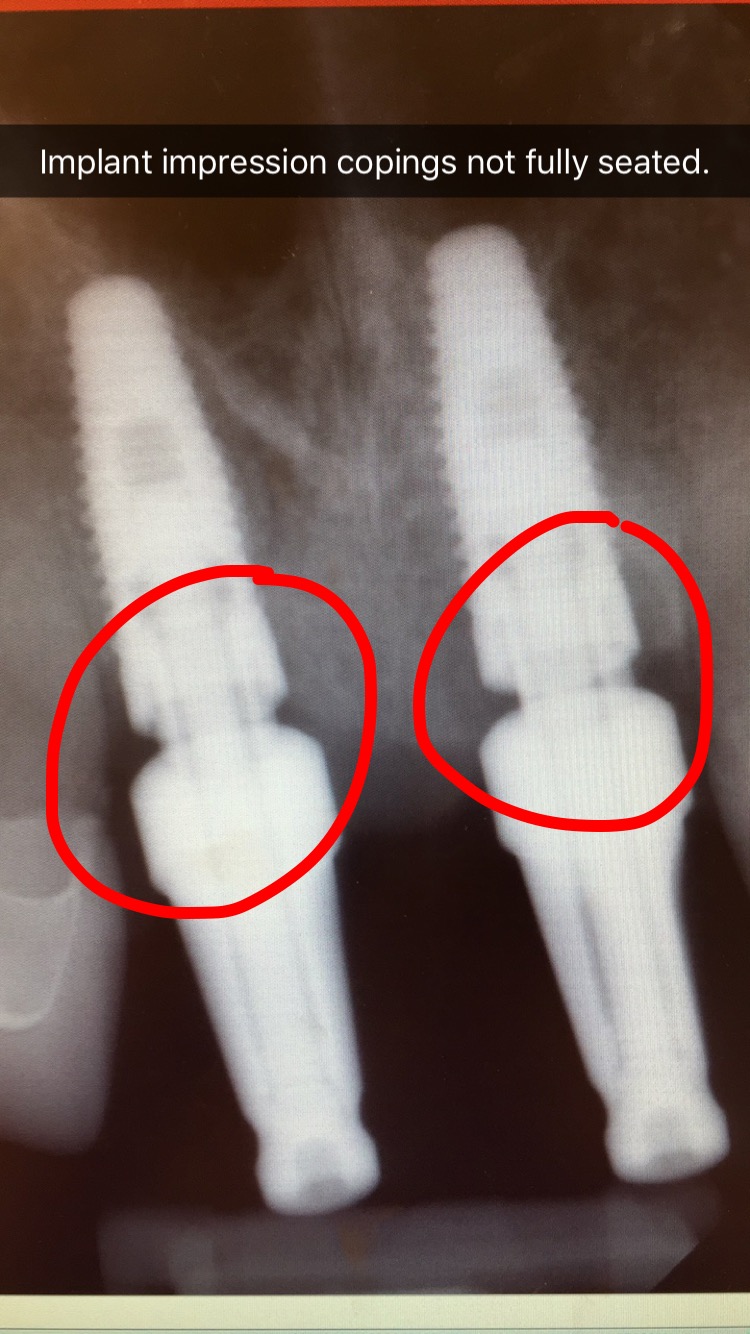
In this case report Dr. Gentry demonstrates the importance of taking a radiograph when seating the custom abutment and crown before final torquing of the gold implant interface connecting screw.





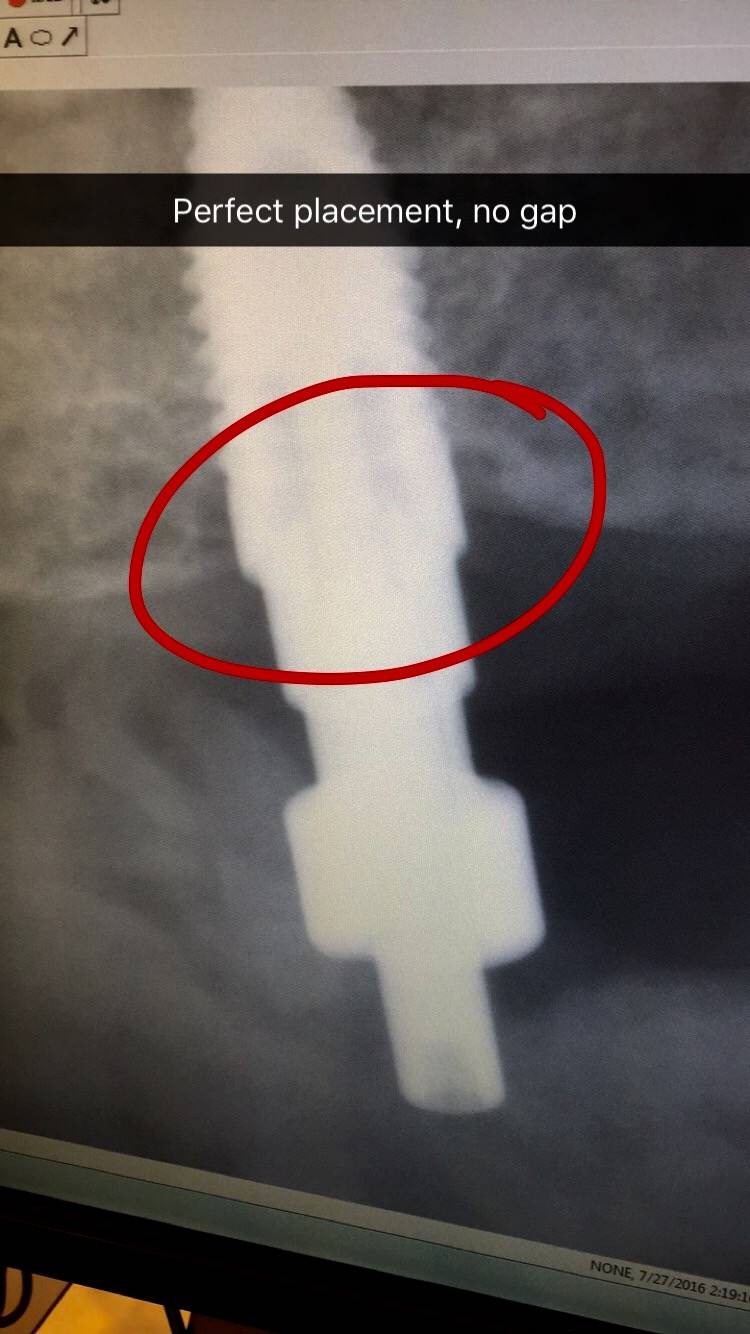
Here’s an example from a case I was doing with a dental student involving the 2 upper front teeth. In the first x-ray the impression copings were not fully seated. I re-positioned the copings and another x-ray was taken to confirm proper alignment. You cannot tell without an x-ray since this is below the gum-line.
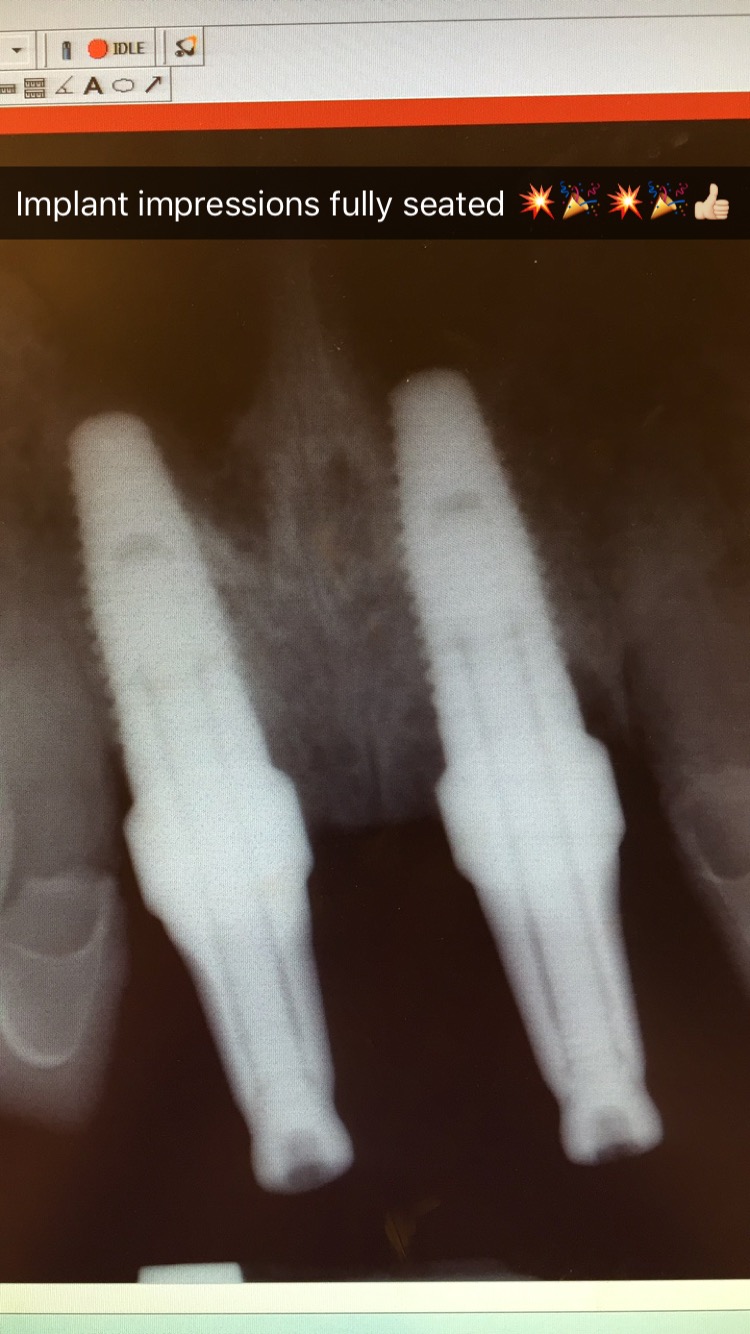
Here’s an example of another implant check x-ray to verify proper seating.